The CDC acknowledged “studies have not yet been done” on pregnant women but they say “experts believe” the COVID vaccine is “unlikely to pose a risk for pregnant people”.
The CDC acknowledged “studies have not yet been done” on pregnant women but they say “experts believe” the COVID vaccine is “unlikely to pose a risk for pregnant people”.The CDC states on their website: “FACT: COVID-19 vaccines do not create or cause variants of the virus that causes COVID-19. Instead, COVID-19 vaccines can help prevent new variants from emerging.”
In senate testimony, CDC Director Dr. Robert Redfield lended insight into possible motivations for such overcounting by reflecting on past experiences with other diseases: “We’ve seen this in other disease processes too… in the HIV epidemic somebody may have a heart attack but also have HIV. The hospital would prefer the DRG [diagnosis-related group] for HIV ‘cause there’s greater reimbursement.” (Source)
COVID hospitalizations among children have always been relatively low, certainly not at a level that can reasonably be considered an “emergency”, especially with the much less virulent Omicron variant.
Some people may argue that a vaccine is needed because even one child dying from COVID is too many.
While it is tragic that some children have died from COVID and that, indeed, even one death is too many, a 0.0003% fatality rate does not constitute an emergency necessitating vaccines that can potentially have fatal or debilitating adverse effects. If the argument, then, is that these effects are extremely rare, the same argument can be made that deaths from COVID among generally healthy children are also extremely rare.
According to analysts in this article: “Covid-19 has killed 280 children under 18 from January through September 2021, the time span in which the alpha and delta variants were active. Flu and pneumonia, heart disease, drowning, guns, and motor vehicles were all deadlier to children during the same time periods annually from 2015 to 2019 (the latest years with available data).”
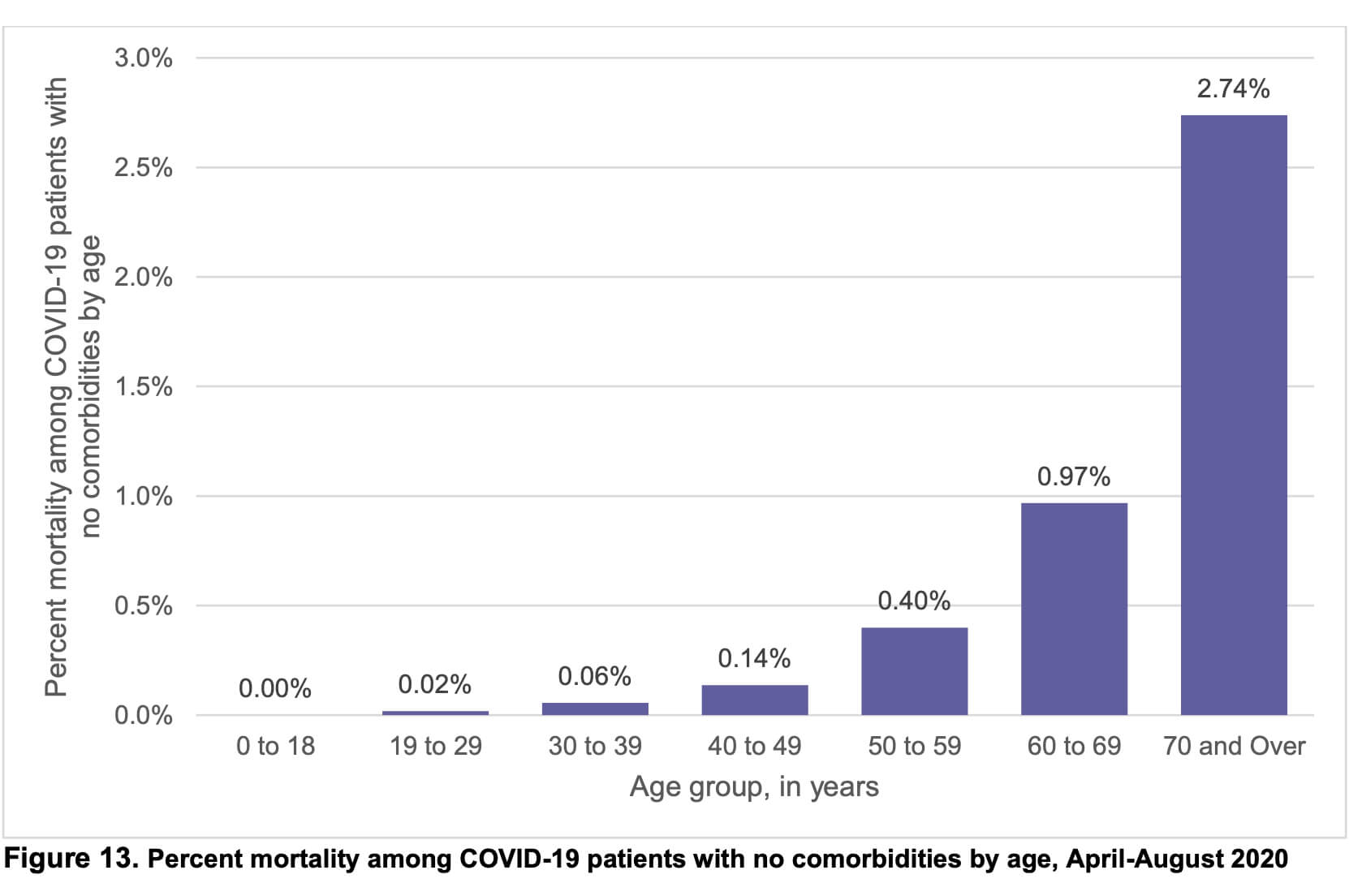
On average, healthy U.S. children ages 0 to 14 are five times more likely to die in a car accident than from COVID-19 (Source). See the chart below.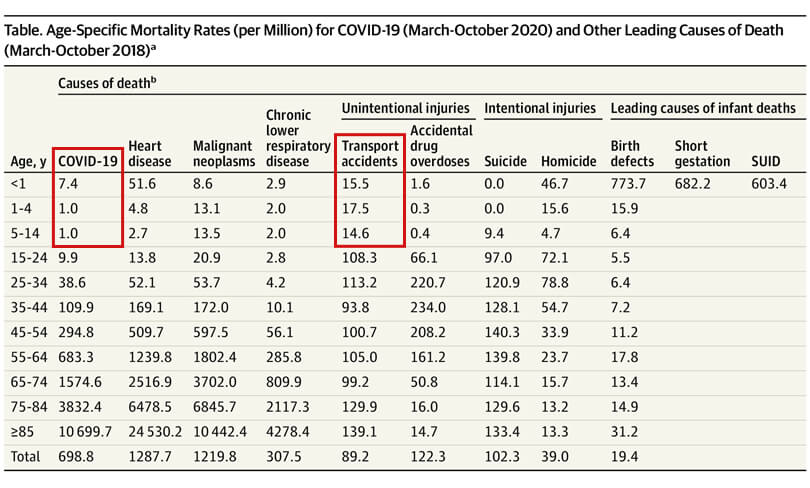 So it seems fair to ask… Why are we not declaring an emergency for children riding in automobiles?
So it seems fair to ask… Why are we not declaring an emergency for children riding in automobiles?
Dr. Scott Jensen said: “I just don’t understand why we are so hell-bent on vaccinating kids under the age of 20 or 30 that have a statistically 0% chance of dying of COVID-19 disease. When we know that there are clearly evidences that this vaccine is problematic in ways we’ve never seen before, wherein the vaccine wasn’t pulled from the market.” (Source at 23:36)
Dr. Richard Fleming, cardiologist, said: “There’s no data that shows [the COVID vaccine] is beneficial for the children.” (Source at 57:04)
Dr. Drew Pinsky said: “Vaccine therapies are usually targeted. They are shingles vaccine for people over the age of 60. It’s pneumonia vaccine for people over the age of 60. I don’t give those to 12 year olds. It’s yellow fever vaccine for people traveling to endemic areas… It doesn’t make any sense to me that [the COVID vaccine] is the one and only vaccine that is completely indiscriminately distributed even though the primary illness is in the adult.” (Source at 1:00:50)
So these questions remain… Where is the COVID emergency for generally healthy children? And if there is no real emergency for them, why are we giving them a vaccine that is meant for emergency use only?



COVID Vaccine Makers Ignore FDA Guidelines
By reporting RRR only and not ARR, the pharmaceutical companies are going against FDA guidance outlined in their official publication entitled Communicating Risks and Benefits: An Evidence-Based User’s Guide.
It states on page 60 that information providers (i.e. doctors, medical professionals, caregivers, etc.) should communicate “absolute risks, not just relative risks. Patients are unduly influenced when risk information is presented using a relative risk approach; this can result in suboptimal decisions. Thus, an absolute risk format should be used.” (Source)
Investigative Journalist Maryanne Demasi says: “It is well established that only quoting RRR without quoting the ARR, can inflate or exaggerate an intervention’s effect size and clinical importance, as well as increase people’s willingness to receive the treatment.” (Source)
Serious Consequences For Health
Gerd Gigerenzer, director of the Harding Center For Risk Literacy, says: “non-transparency is often a deliberate tactic to manipulate or persuade people… Many physicians, patients, health journalists and politicians do not understand health statistics. This collective statistical illiteracy has resulted in serious consequences for health.” (Source)
Dr. Ronald B. Brown, Ph.D said: “Such examples of outcome reporting bias mislead and distort the public’s interpretation of COVID-19 mRNA vaccine efficacy and violate the ethical and legal obligations of informed consent.” (Source)